



You’re 42. You notice your jeans fit differently—specifically, tighter around the middle despite eating the same as always. Your sleep is disrupted. You’re more fatigued. Your periods are becoming irregular. Your mood fluctuates more than it used to.
Your GP says “this is perimenopause—it’s normal.” But nobody tells you what to actually do about it.
Here’s what usually happens: you try the strategies that worked in your 20s and 30s—more cardio, eating less. You run more, cycle longer, attend more fitness classes. Yet your body composition continues shifting. You’re exhausted from all the extra cardio. The weight gain continues. You feel frustrated and confused.
The problem isn’t lack of effort—it’s using the wrong approach for a body experiencing hormonal changes that dramatically affect how it responds to exercise and nutrition.
I’m Will Duru, a personal trainer with over 10 years’ experience in London. I’ve coached dozens of women through perimenopause and menopause, and the transformation that occurs when they switch from cardio-focused training to proper strength training is remarkable.
This guide explains exactly what happens to your body during perimenopause and menopause, why strength training becomes essential (not optional) after 40, what specific benefits strength training provides for hormonal changes, how to start strength training safely if you’re new, and how 12REPS programmes workouts specifically for women over 40.

Understanding Perimenopause and Menopause
The Timeline
According to Women’s Health UK’s comprehensive menopause guide, the transition typically follows this pattern:
Perimenopause (The Transition Phase):
- Typically begins: Ages 40-47 (can start earlier)
- Duration: 4-10 years (average 4-6 years)
- What happens: Hormone levels (oestrogen, progesterone) fluctuate erratically
- Periods: Irregular, varying cycle lengths
- Still fertile (though declining): Pregnancy still possible
Menopause (The Moment):
- Definition: 12 consecutive months without a period
- Average age: 51 (UK), range 45-55
- Technically a single point in time, not a phase
Postmenopause (After Menopause):
- Begins: After 12 months without a period
- Duration: Rest of life
- Hormone levels: Stabilised at low levels
- Symptoms: Often improve but some persist
This guide focuses on perimenopause and early postmenopause—the 10-15 year window where strategic exercise intervention makes the biggest difference.
What’s Happening Hormonally
Oestrogen decline:
- Drops gradually through perimenopause
- Reaches very low levels postmenopause
- Never returns to premenopausal levels
Why this matters for training:
- Oestrogen regulates muscle protein synthesis (building muscle)
- Oestrogen maintains bone density
- Oestrogen influences fat distribution (where you store fat)
- Oestrogen affects insulin sensitivity (how you process carbohydrates)
- Oestrogen impacts recovery capacity
Progesterone decline:
- Also drops through perimenopause
- Affects sleep quality, mood stability, stress response
The result: Your body’s response to exercise, nutrition, and recovery fundamentally changes.
Common Physical Changes
The North American Menopause Society identifies these typical changes:
Body composition shifts:
- Loss of muscle mass (sarcopenia): 3-8% per decade after 30, accelerating after menopause
- Increased fat mass, particularly visceral fat (belly fat)
- Changes in fat distribution: less in hips/thighs, more in abdomen
- Total weight gain: Average 0.5-1kg annually through perimenopause
Metabolic changes:
- Decreased resting metabolic rate (burn fewer calories at rest)
- Reduced insulin sensitivity (higher risk of type 2 diabetes)
- Changes in cholesterol profile (increased cardiovascular risk)
Musculoskeletal changes:
- Accelerated bone density loss (up to 20% lost during transition)
- Increased risk of osteoporosis and fractures
- Joint pain and stiffness
- Reduced flexibility
Other symptoms affecting training:
- Hot flushes and night sweats (disrupt sleep, reduce training capacity)
- Fatigue and reduced energy
- Brain fog (affects motivation and focus)
- Mood changes (depression, anxiety, irritability)

Why Strength Training Becomes Essential After 40
The exercise approach that worked in your 20s and 30s doesn’t work the same way in your 40s and beyond. Here’s why strength training specifically becomes critical.
Reason 1: Prevents Muscle Loss (Sarcopenia)
What research shows: According to a comprehensive review in PMC on exercise beyond menopause, women lose 3-8% of muscle mass per decade after age 30, with accelerated loss during and after menopause due to declining oestrogen.
Why this matters:
- Less muscle = lower metabolic rate (burn fewer calories at rest)
- Less muscle = reduced functional capacity (daily tasks become harder)
- Less muscle = increased fall risk and frailty
What strength training does: Research published in the Journal of Mid-life Health demonstrates that resistance training 2-3x weekly not only prevents muscle loss but can actually build new muscle mass, even in women over 60.
The key: Progressive resistance training provides the stimulus needed to maintain and build muscle despite declining oestrogen.
Reason 2: Protects Bone Density
What happens naturally: Up to 20% of bone loss occurs during the 5-7 year perimenopause/early postmenopause window. This dramatically increases osteoporosis and fracture risk.
Why cardio doesn’t solve this: Walking, cycling, swimming don’t provide sufficient mechanical load to stimulate bone remodelling.
What strength training does: Research shows that progressive resistance training—particularly exercises involving heavy loads on major muscle groups—creates mechanical stress that signals bones to rebuild and strengthen.
Critical finding: Studies show strength training at 80% of one-rep max (heavy enough that you can only complete 8-12 reps), performed 2x weekly, significantly improves bone mineral density in postmenopausal women.
Best exercises for bone health:
- Squats (load spine and hips)
- Deadlifts (load spine, hips, entire posterior chain)
- Lunges (load hips unilaterally)
- Overhead press (load spine and shoulders)
These are precisely the exercises 12REPS programmes.
Reason 3: Improves Metabolic Health and Body Composition
The problem: Declining oestrogen reduces insulin sensitivity and shifts fat distribution toward visceral (abdominal) fat—the most dangerous type, associated with cardiovascular disease, diabetes, and inflammation.
Why more cardio often fails: Excessive cardio without adequate strength training can actually accelerate muscle loss, worsening metabolic health.
What strength training does:
According to research reviewed in Sports Medicine, resistance training:
- Improves insulin sensitivity (better blood sugar control)
- Reduces visceral fat specifically (not just total fat)
- Increases resting metabolic rate (more muscle = burn more calories at rest)
- Improves lipid profile (HDL up, LDL and triglycerides down)
Practical impact: Women who strength train through perimenopause typically gain less abdominal fat and maintain more stable weight than those doing cardio only.
Reason 4: Reduces Menopausal Symptoms
Surprising finding: Research shows strength training directly improves several menopausal symptoms beyond just body composition.
Symptoms improved by strength training:
Hot flushes and night sweats: Studies suggest regular resistance exercise reduces frequency and severity, possibly through improved thermoregulation and reduced stress hormones.
Sleep quality: Research demonstrates strength training improves sleep duration and quality in postmenopausal women, likely through reduced anxiety and improved stress response.
Mood and mental health: Resistance training reduces depression and anxiety symptoms, improves self-esteem and body image, and enhances overall quality of life.
Brain fog: Exercise improves cognitive function and may protect against cognitive decline associated with menopause.
Joint pain: Strengthening muscles around joints reduces pain and improves function.
Reason 5: Maintains Functional Independence
The long game: Strength training in your 40s and 50s determines your functional capacity in your 70s and 80s.
What functional independence means:
- Carrying shopping bags
- Getting up from the floor
- Climbing stairs without breathlessness
- Playing with grandchildren
- Travelling independently
- Living in your own home (not requiring care)
Research shows: Women who strength train regularly through menopause maintain significantly better functional capacity 20-30 years later compared to those who don’t.
This isn’t about vanity—it’s about quality of life for the next 40+ years.

Common Concerns About Strength Training After 40
Concern 1: “I’ll get bulky”
Reality: Building significant muscle mass becomes harder, not easier, as oestrogen declines. Oestrogen supports muscle protein synthesis—with less oestrogen, your capacity to build large amounts of muscle is actually reduced.
What actually happens: You build lean, functional muscle that creates a toned, defined appearance. The “bulky” look requires years of dedicated bodybuilding with extremely high volume and often performance-enhancing drugs—it doesn’t happen accidentally.
More likely: You’ll feel stronger, look more defined, and your clothes will fit better.
Concern 2: “I’m too old to start”
Reality: It’s never too late to start strength training and see benefits.
Research confirms that women can build muscle and strength at any age. Studies show women in their 60s, 70s, and 80s who begin strength training make significant gains in muscle mass, strength, and bone density.
Starting at 42 vs 52 vs 62: All produce benefits. Earlier is better, but late is better than never.
Concern 3: “I need medical clearance first”
When medical clearance IS required:
- Cardiovascular conditions (heart disease, uncontrolled hypertension)
- Recent surgery or injury
- Osteoporosis diagnosis (need modified programme)
- Any condition causing concern
When you can start without clearance:
- Generally healthy with no diagnosed conditions
- Cleared for normal daily activities
- No cardiovascular symptoms (chest pain, significant breathlessness)
Sensible approach: If you have any doubts, consult your GP. But for most healthy women over 40, beginning a progressive strength training programme is safe.
Concern 4: “My joints hurt—won’t weights make it worse?”
Reality: Appropriate strength training typically improves joint pain, not worsens it.
Why joints hurt: Often due to weak muscles failing to support and stabilise the joint properly. Strengthening surrounding muscles reduces joint stress.
Key qualifier: “Appropriate” strength training means:
- Starting with manageable loads
- Progressing gradually
- Using proper form
- Working within pain-free ranges of motion
Avoid: Jumping into heavy weights immediately, using poor form, training through sharp pain.
If you have diagnosed arthritis or joint conditions: Work with a physiotherapist initially to learn appropriate modifications.

How to Start Strength Training After 40 (If You're New)
Phase 1: Weeks 1-4 (Learning Phase)
Goal: Learn fundamental movement patterns with minimal load. Build exercise habit.
Frequency: 2x weekly (e.g., Monday and Thursday)
Format: Full body workouts
Load: Bodyweight or very light weights (2-5kg dumbbells)
Exercises to master:
- Bodyweight squats
- Glute bridges
- Press-ups (wall or incline if needed)
- Bodyweight rows (using TRX or table)
- Plank holds
- Bodyweight lunges
Sets × Reps: 2-3 sets × 10-12 reps
Rest between sets: 90-120 seconds
What to expect: Moderate soreness initially (normal DOMS), gradual improvement in movement quality, building confidence.
Phase 2: Weeks 5-12 (Building Phase)
Goal: Increase load gradually while maintaining good form. Build strength base.
Frequency: 2-3x weekly
Load progression: Increase weight when you can complete all sets with good form. Typical increases: 2-5kg for lower body, 1-2kg for upper body.
Example progression for squats:
- Week 5: Bodyweight × 12 reps
- Week 7: Goblet squat 8kg × 10 reps
- Week 9: Goblet squat 12kg × 10 reps
- Week 11: Barbell squat 20kg (empty bar) × 8 reps
What to expect: Noticeable strength gains, reduced soreness, increased confidence with heavier weights, beginning to see body composition changes.
Phase 3: Weeks 13-24 (Progression Phase)
Goal: Continue progressive overload systematically. Establish long-term training habit.
Frequency: 2-4x weekly (depending on schedule and recovery)
Load: Working with challenging weights that allow 8-12 reps with good form
Programming options:
- 2x weekly: Full body both sessions
- 3x weekly: Full body all sessions OR Upper/Lower/Full
- 4x weekly: Upper/Lower/Upper/Lower split
What to expect: Significant strength improvements (often 50-100% increase in weights lifted from week 1), visible muscle definition, improved body composition, established exercise habit.
Phase 4: Weeks 25+ (Long-term Training)
Goal: Maintain progressive overload indefinitely. Training becomes lifestyle, not temporary intervention.
This is where 12REPS becomes particularly valuable—providing structured progression that continues for months and years, not just weeks.

What Makes 12REPS Suitable for Women Over 40
Appropriate Volume and Frequency
Why this matters: Recovery capacity decreases with age. What worked at 25 (training 6x weekly, very high volume) often creates excessive fatigue at 45.
What 12REPS does:
- Programmes 2-4 training sessions weekly (you choose based on your schedule)
- Sets volume appropriately for recovery capacity
- Includes built-in deload weeks every 5-8 weeks (reduces accumulated fatigue)
Result: Enough training stimulus to build muscle and strength without compromising recovery or causing burnout.
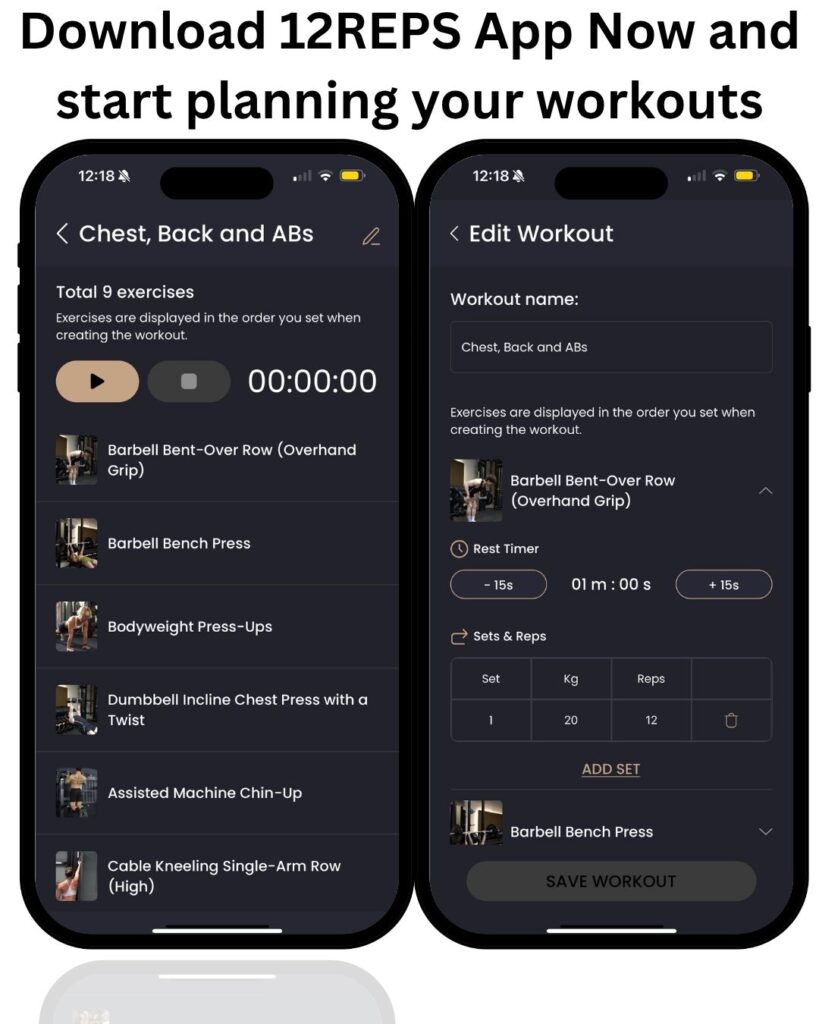
Progressive Overload Without Guesswork
Why this matters: You need to progressively increase weights/reps to continue building muscle and bone density. But jumping too fast increases injury risk.
What 12REPS does:
- Tracks your performance every session
- Automatically suggests weight increases when you’re ready
- Progresses you gradually (typically 2.5-5kg increases for lower body, 1-2kg for upper body)
- Adjusts progression rate based on your actual performance
Result: Consistent progression without overreaching or plateauing.
Exercise Selection for Bone and Muscle Health
Why this matters: Not all exercises provide equal benefit for bone density and functional strength.
What 12REPS prioritises:
What 12REPS prioritises:
- Compound lifts that load multiple muscle groups and bones (squats, deadlifts, presses, rows)
- Exercises proven to improve bone mineral density
- Functional movement patterns (movements used in daily life)
Result: Maximum benefit per session—building muscle, bone density, and functional strength simultaneously.
Equipment Flexibility
Why this matters: You might train at a gym, at home with minimal equipment, or a combination.
What 12REPS offers:
- Gym programmes (full equipment access)
- Home programmes (dumbbells only or bodyweight only)
- Hybrid programmes (gym some days, home others)
- Programme adjusts based on equipment available
Result: Can maintain training consistency regardless of circumstances (travel, gym closures, schedule changes).
Video Demonstrations for Every Exercise
Why this matters: Proper form becomes even more critical after 40 to prevent injury.
What 12REPS provides:
- 1,500+ exercise video library
- Multiple angles for complex movements
- Form cues and common mistakes highlighted
Result: Confidence in performing exercises correctly, reduced injury risk.
Realistic Time Commitment
Why this matters: You’re busy—career, possibly children, aging parents, responsibilities. Training can’t dominate your schedule.
What 12REPS delivers:
- 30-45 minute sessions (not 90-minute marathon workouts)
- Efficient programming (no wasted time on ineffective exercises)
- Sustainable long-term (doesn’t require clearing your entire schedule)
Result: Maintainable training habit that fits real life.
Sample 12REPS Training Week (Women Over 40, 3 Days Weekly)
This represents a typical training week for a woman who’s completed the initial 12-24 week learning phase.
Monday: Lower Body Focus
- Barbell Back Squats: 4 sets × 8-10 reps @ 50kg
- Romanian Deadlifts: 3 sets × 10-12 reps @ 40kg
- Walking Lunges: 3 sets × 10 reps each leg @ 10kg dumbbells
- Glute Bridges: 3 sets × 12-15 reps @ 30kg
- Plank: 3 sets × 45-60 seconds
Session duration: 40 minutes
Wednesday: Upper Body Focus
- Barbell Bench Press: 4 sets × 8-10 reps @ 30kg
- Bent Over Rows: 4 sets × 8-10 reps @ 35kg
- Overhead Press: 3 sets × 10-12 reps @ 20kg
- Lat Pulldowns: 3 sets × 10-12 reps @ 35kg
- Bicep Curls: 2 sets × 12-15 reps @ 8kg dumbbells
- Tricep Extensions: 2 sets × 12-15 reps @ 12kg
Session duration: 40 minutes
Friday: Full Body
- Deadlifts: 4 sets × 6-8 reps @ 60kg
- Incline Dumbbell Press: 3 sets × 10-12 reps @ 12kg dumbbells
- Bulgarian Split Squats: 3 sets × 10 reps each leg @ 14kg dumbbells
- Cable Rows: 3 sets × 10-12 reps @ 30kg
- Lateral Raises: 3 sets × 12-15 reps @ 6kg dumbbells
- Face Pulls: 3 sets × 15 reps @ 15kg
Session duration: 45 minutes
Total weekly training time: 125 minutes (just over 2 hours)
This provides sufficient stimulus for:
- Maintaining and building muscle mass
- Improving or maintaining bone density
- Improving metabolic health
- Building functional strength

Nutrition Considerations for Women Over 40
Protein Requirements Increase
Why: Declining oestrogen reduces muscle protein synthesis efficiency. You need more protein per kg bodyweight to achieve the same muscle-building effect.
Recommendation:
- Age 20-40: 1.6-1.8g/kg bodyweight sufficient
- Age 40+: 1.8-2.2g/kg bodyweight recommended
- Age 50+: 2.0-2.4g/kg bodyweight ideal
Example for 65kg woman over 40:
- Minimum: 117g protein daily
- Optimal: 130-143g protein daily
Why this matters: Inadequate protein + strength training = minimal muscle gain, poor recovery.
Calorie Needs Change
The reality: Your resting metabolic rate declines with age and declining muscle mass. You need fewer calories than you did at 25.
However: Severe calorie restriction whilst strength training is counterproductive—you need adequate calories to build muscle.
Approach:
If maintaining weight:
- Eat at maintenance calories (bodyweight in kg × 30-32)
- Prioritise protein
- Allow gradual body recomposition (lose fat, gain muscle over 6-12 months)
If losing fat:
- Moderate deficit only (300-400 calories below maintenance)
- Maintain high protein (2.0-2.2g/kg)
- Accept slower fat loss to preserve muscle
- Expect 0.25-0.5kg loss weekly maximum
If building muscle:
- Slight surplus (200-300 calories above maintenance)
- High protein
- Accept some fat gain is normal
- Aim for 0.5-1kg gain monthly
Perimenopause-Specific Nutrition Challenges
Challenge 1: Increased cravings and hunger
Why: Hormone fluctuations affect appetite regulation.
Strategy: Prioritise protein and fibre at every meal (maximises satiety), structured meal times (reduces grazing), adequate sleep (poor sleep increases hunger hormones).
Challenge 2: Digestive changes
Why: Declining oestrogen affects gut motility and microbiome.
Strategy: Increase fibre gradually, prioritise fermented foods, consider probiotic supplement, adequate hydration.
Challenge 3: Alcohol tolerance decreases
Why: Reduced oestrogen affects alcohol metabolism.
Reality: You’ll likely find alcohol affects sleep, recovery, and body composition more significantly than it did in your 30s. Consider reducing frequency and quantity.
Real Client Example: Sarah, Age 46
Background:
- Perimenopause for 2 years (irregular periods, night sweats, weight gain)
- Always been “cardio person” (running, spin classes)
- Gained 6kg over 18 months despite running more
- Never lifted weights
Starting point (Month 1):
- Weight: 72kg
- Squat: Bodyweight only (couldn’t squat to parallel with empty bar)
- Deadlift: 20kg (empty bar)
- Bench press: 15kg (fixed barbell)
Programme:
- Started 12REPS 2x weekly full body
- Gradually increased to 3x weekly by month 3
- Continued running but reduced to 2x weekly (from 5x)
Results after 12 months:
- Weight: 69kg (lost 3kg)
- Body composition: Visibly more muscular, lost 2 dress sizes despite only 3kg total weight loss
- Squat: 65kg × 8 reps
- Deadlift: 80kg × 6 reps
- Bench press: 40kg × 8 reps
Reported benefits:
- Better sleep (night sweats reduced significantly)
- Improved mood and energy
- More confident
- Clothes fit better despite similar weight
- Stronger in daily life (carrying shopping, moving furniture, gardening)
Key insight: The switch from cardio-dominant to strength-focused training, combined with increased protein intake (from ~80g to 130g daily), produced better results in 12 months than 2 years of additional running had achieved.

The Bottom Line
Strength training isn’t optional for women over 40—it’s essential medicine for the hormonal changes your body is experiencing.
What happens naturally during perimenopause and menopause:
❌ Muscle mass declines (3-8% per decade, accelerating postmenopause)
❌ Bone density decreases rapidly (up to 20% loss during transition)
❌ Fat increases and redistributes to abdomen (visceral fat)
❌ Metabolic rate declines
❌ Insulin sensitivity worsens
❌ Functional capacity declines
What strength training does:
✅ Prevents muscle loss and builds new muscle (even with declining oestrogen)
✅ Protects and improves bone density (particularly with heavy loads 80%+ of 1RM)
✅ Improves body composition (lose fat, gain muscle)
✅ Improves metabolic health (insulin sensitivity, lipid profile)
✅ Reduces menopausal symptoms (hot flushes, mood, sleep, brain fog)
✅ Maintains functional independence long-term
Critical evidence:
- Studies show 2x weekly strength training significantly improves muscle mass, bone density, and metabolic health in postmenopausal women
- Strength training at 80% intensity (heavy enough for 8-12 reps) provides optimal bone benefits
- Women can build muscle at any age—it’s never too late to start
- Cardio alone does not prevent muscle loss or bone density decline
How to start:
✅ Begin with 2x weekly, full body workouts
✅ Learn fundamental patterns (squats, deadlifts, presses, rows)
✅ Progress load gradually (2.5-5kg increases when ready)
✅ Prioritise protein (1.8-2.2g/kg bodyweight)
✅ Be patient—significant changes take 6-12 months
How 12REPS helps:
✅ Programmes appropriate volume and frequency (2-4x weekly based on your schedule)
✅ Progressive overload automatically managed (no guesswork on when to increase weight)
✅ Exercise selection optimised for bone/muscle health
✅ Video demonstrations for proper form (1,500+ exercises)
✅ Equipment flexibility (gym/home/hybrid)
✅ 30-45 minute efficient sessions (sustainable long-term)
✅ Built-in deload weeks (manages recovery for women over 40)
Try 12REPS free for 7 days. Start building the muscle and bone density that will serve you for the next 40+ years.
The women who thrive through menopause and beyond aren’t those doing more cardio—they’re those who prioritised strength training in their 40s and 50s, building a foundation of muscle and bone that protects their health, function, and independence for decades.
Start today. Your 60, 70, and 80-year-old self will thank you.
References
- Maltais, M.L., Desroches, J. and Dionne, I.J. (2009). Changes in Muscle Mass and Strength after Menopause. Journal of Musculoskeletal and Neuronal Interactions, 9(4), pp.186-197.
- Bondarev, D., Laakkonen, E.K., Finni, T., Kokko, K., Kujala, U.M., Aukee, P., Kovanen, V., Sipilä, S. and Laakkonen, E.K. (2018). Physical Performance in Relation to Menopause Status and Physical Activity. Menopause, 25(12), pp.1432-1441. https://doi.org/10.1097/GME.0000000000001137
- Capel-Alcaraz, A.M., García-López, H., Castro-Sánchez, A.M., Fernández-Sánchez, M., Lara-Palomo, I.C. and Matarán-Peñarrocha, G.A. (2023). The Efficacy of Strength Exercises for Reducing the Symptoms of Menopause: A Systematic Review. Journal of Clinical Medicine, 12(3), 751. https://doi.org/10.3390/jcm12030751
- Sternfeld, B., Wang, H., Quesenberry, C.P., Abrams, B., Everson-Rose, S.A., Greendale, G.A., Matthews, K.A., Torrens, J.I. and Sowers, M. (2004). Physical Activity and Changes in Weight and Waist Circumference in Midlife Women: Findings from the Study of Women’s Health Across the Nation. American Journal of Epidemiology, 160(9), pp.912-922. https://doi.org/10.1093/aje/kwh299
- Kohrt, W.M., Bloomfield, S.A., Little, K.D., Nelson, M.E. and Yingling, V.R. (2004). Physical Activity and Bone Health. Medicine & Science in Sports & Exercise, 36(11), pp.1985-1996. https://doi.org/10.1249/01.MSS.0000142662.21767.58

{kind=link}
{kind=link}